
Achilles Tendonitis
OVERVIEW
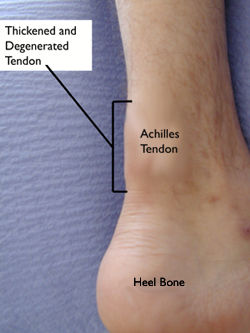
ANATOMY
- Annual incidence of Achilles tendinopathy is between 7% - 9%.
- Mean age of injury is 30 – 50 year old
- Males > Females
- Majority are individuals engaging in activity but a minority of the cases has been reported in the sedentary
- Runners most commonly affected
- Symptoms more likely to appear during training rather than during competitive events
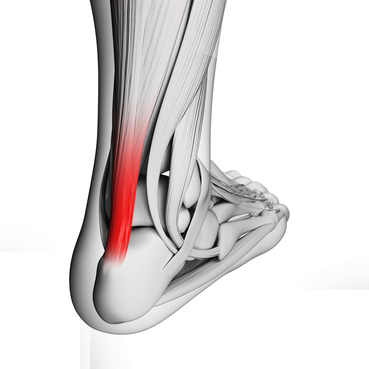
ANATOMY
- Achilles tendon is the largest and strongest tendon in the body
- Avg. length is approximately 15 cm
- Serves as the tendon for BOTH the gastrocnemius and soleus
- PROXIMALLY the tendon is broad and flat – then is becomes more narrow and rounded – until it flattens out when it inserts on the posterior surface of the calcaneus.
RISK FACTORS
Intrinsic
Extrinsic
Intrinsic
- Abnormal DF ROM (Increased or Decreased)
- Abnormal Subtalar ROM (increased or Decreased)
- Decreased PF strength
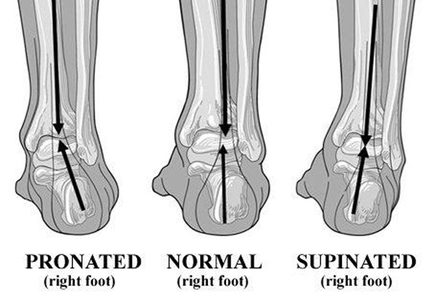
- Increased Pronation
- Tendon structure (determined by ultrasound signal)
- Comorbidities (obesity, hypertension, high cholesterol, and diabetes)
Extrinsic
- Training errors (sudden increase in duration/intensity, hill training)
- Faulty equipment (poor shoes, etc…)
- Environmental factors (winter > summer)
|
DIAGNOSIS
SIGNS AND SYMPTOMS
Positive when tenderness w/ ankle in slight PF that decreases as ankle is DF |
|

TESTS
Royal London Hospital Test
Royal London Hospital Test
- Examiner palpates the area of the tendon most tender. Patient actively dorsiflexes and the examiner palpates the tendon again in max dorsiflexion.
- Positive when tendon is less tender in max dorsiflexion
Arc Sign
- Patient is asked to actively dorsiflex and plantarflex and the examiner looks to see if the area of maximal localized swelling moves or remains static
- Positive if the area moves proximally and distally
References:
- Carcia CR, Martin RL, Houck J, Wukich DK. Achilles pain, stiffness, and muscle power deficits: achilles tendinitis. J Orthop Sports Phys Ther. 2010;40(9):A1-26.
Last Edited by: Jason Greenwood , SPT at AT Still University on July 10, 2014
