
Plantar Fasciitis

Overview:
Pathoanatomical Features:
Plantar aponeurosis or fascia consist of 3 bands
Risk Factors:
Diagnosis/Classification:
Physical Examination Measures:
Palpation of the proximal plantar fascia insertion:
- Second most common foot condition treated by healthcare providers
- Occurs in approximately 2 million Americans each year
- Affects as much as 10% of the US population over the course of a lifetime
- Prevalent in both athletic and nonathletic populations
- Most common in ages 40 - 60 years old
Pathoanatomical Features:
Plantar aponeurosis or fascia consist of 3 bands
- Lateral, medial, and central
- Central band originates from medial tubercle on plantar surface of the calcaneus and inserts to the metatarsal heads as 5 slips
- Each slip bifurcates to insert on the proximal phalanx of each toe
- The plantar fascia is shortened when the toes are extended
Risk Factors:
- High body mass index in nonathletic populations
- Decreased ankle dorsiflexion
- Decreased posterior leg muscle length
- Spending majority of workday on feet
- Activities placing increased load on heel and attached tissues (long distance running, ballet dancing, etc.)
Diagnosis/Classification:
- Pain under plantar surface of heel upon weight bearing after a period of non-weight bearing
- Insidious onset
- Pain most noticeable with first steps in morning or after a period of inactivity
- Pain may result in antalgic gait
- Pain decreases with activity (walking, running, etc.) but worsen toward the end of the day
- History of change in activity level – increased distance for running/walking, employment change with more time on their feet
- Initial complaint of sharp, localized pain at anteromedial aspect of plantar surface of heel, with paresthesias being uncommon
Physical Examination Measures:
- Palpation of the proximal plantar fascia insertion
- Active and passive talocrural joint dorsiflexion ROM
- Tarsal tunnel syndrome test
- Windlass test
- The longitudinal arch angle
Palpation of the proximal plantar fascia insertion:
- Palpation at the origin where fascia attaches to the medial tubercle of the calcaneus to asses for symptoms of pain or tenderness

Active and passive talocrural joint dorsiflexion ROM:
- The amount of ankle dorsiflexion ROM with knee extended
- Patient is in prone with feet over edge of table
- Patient actively or PT passively dorsiflexes ankle
- PT makes sure that foot does not invert or evert
- Goniometer measurement taken lining up along the fibula and 5th metatarsal

Dorisflexion-Eversion test for Tarsal Tunnel Syndrome:
- In non-weight bearing, dorsiflexion of ankle, eversion of foot, and extension of all toes maintained for 5-10 seconds to elicit symptoms
- Patient in sitting
- PT maximally dorsiflexes ankle, everts foot, and extends toes for 5-10 secs.
- PT taps over the region of the tarsal tunnel during the 5-10 hold duration
- Determines if a positive Tinel sign is present or if patient complains of local nerve tenderness
Windlass Test:
- Extension of first metatarsophalangeal joint in both weight bearing and non-weight bearing to cause windlass effect of plantar fascia and if patient’s heel pain is reproduced
- Non-weight bearing
- PT extends first metatarsophalangeal joint to end of range or pain reproduced
- Weight bearing
- PT extends first metatarsophalangeal joint to end of range or pain reproduced
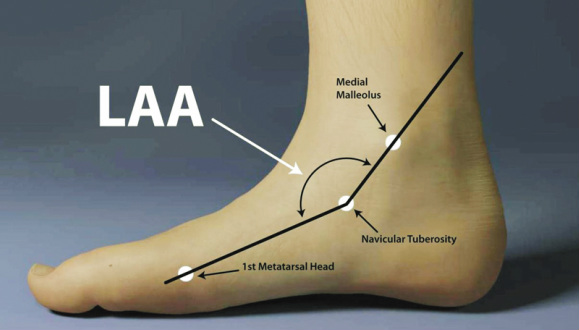
Longitudinal Arch Angle:
- The angle formed by a line from the midpoint of the medial malleolus to the navicular tuberosity in relation to another line projected from the most medial prominence of the first metatarsal head to the navicular tuberosity
- Patient is standing with equal weight on both feet
- Palpation of the medial malleolus, navicular tuberosity, and most medial prominence of the first metatarsal head are marked with pen
- A goniometer measurement is taken with the axis at the navicular tuberosity
References:
- Mcpoil TG, Martin RL, Cornwall MW, Wukich DK, Irrgang JJ, Godges JJ. Heel pain--plantar fasciitis: clinical practice guildelines linked to the international classification of function, disability, and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38(4):A1-A18.
Last Edited by: Joseph Kauffman, SPT at AT Still University on July 12, 2014
